
Anesthesia and Pyometra. What Now?
Escrito por: Luisa Yamamoto e Adriano Carregaro
What is pyometra?
Pyometra is a common disease in female dogs, especially those that are not spayed, starting from 8 years of age, and it usually occurs in association with another uterine condition called cystic endometrial hyperplasia.
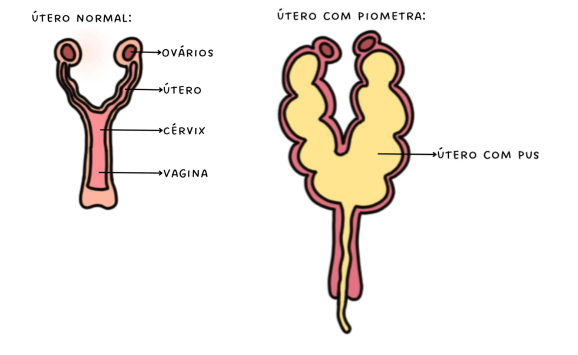
Pyometra usually occurs during diestrus, around two months after estrus, when the concentration of progesterone is high. Progesterone acts on the uterus by stimulating the growth of uterine glands, mucous secretion within this organ, reducing uterine contractions, decreasing the immune response locally, and closing the cervix. This leads to the accumulation of fluids inside the uterus, creating a favorable environment for bacterial colonization (especially by E. coli). Females with pyometra have the uterus filled with pus (Figure 1), and they may appear lethargic, with purulent vulvar discharge present or absent, abdominal pain, fever, among other clinical signs.
Treatment and main concerns
Pyometra is typically an emergency situation because the immune response is compromised and progesterone prevents uterine contractions to expel the contents. Therefore, in a short period, the dog can develop sepsis (widespread infection), affecting various other organs and increasing the risk of mortality. Therefore, the faster pyometra is identified and treated, the lower the chances of complications and death.
Treatment for pyometra is preferably surgical, through spaying. Because it is a serious infectious process, pyometra alters various parameters, making the anesthetic procedure somewhat complicated. Among the main changes are anemia, dehydration, decreased perfusion, liver and kidney alterations, deposition of immune complexes in the renal glomerulus, and action of bacterial endotoxins in the renal tubules. Additionally, patients with pyometra often present with tachycardia, tachypnea, hypotension, and metabolic acidosis. To delve deeper into the etiology and main consequences of pyometra, refer to the "Find out more" section at the end of this post.
Stabilization
Whenever possible, hydration and volemia should be corrected before the procedure to stabilize the patient, prevent shock and hypotension, and increase renal perfusion. The fluid therapy rate can be more conservative (5 mL/kg/h) or even slightly more liberal (up to 10 mL/kg/h), depending on the level of dehydration and colloid osmotic pressure of the patient. You can learn more about the different forms of fluid correction in patients with pyometra at this link.
Another important point is to correct the acid-base imbalance. To do this, it is ideal to perform a blood gas analysis and assess the patient's acid-base status, paying attention to pH, SaO2, PaCO2, HCO3–, íons de sódio, potássio e cloreto, ânion gap base excess. Since these patients are usually in a state of metabolic acidosis, it is important to use a fluid therapy with HCO3, which means using lactated Ringer's solution with the addition of sodium bicarbonate.
Anesthesia
It's interesting that the premedication includes analgesic drugs such as opioids, avoiding phenothiazine tranquilizers (like acepromazine) due to their hypotensive effect and decreased myocardial contractility. Another option for pre-anesthetic medication is dexmedetomidine, a drug widely used in the pre-anesthetic medication of these patients.
The induction can be done with etomidate or propofol (with co-inducers) in stable patients who have preferably received fluid resuscitation in the pre-anesthetic period. Additionally, induction can also be performed with inhalation anesthetics via a mask in more debilitated patients with advanced shock and/or hypotension. Ketamine can also be used, associated with a muscle relaxant. However, this modality does not enable more invasive and bloody procedures, such as OSH (ovariohysterectomy), indicating that dissociative anesthetics should not be the mainstay of maintenance but can be used in infusion form to enhance and assist in general anesthesia.
For the same reasons, maintenance is preferably done with isoflurane or sevoflurane. However, like all other anesthetic modalities, inhalation anesthesia can exacerbate hypotension, so the association of continuous infusion analgesics such as opioids, dexmedetomidine, or ketamine will provide analgesia and enhance anesthesia, reducing the requirement for inhalation anesthetics and thus avoiding the occurrence of their undesirable effects.
Maintenance can also be done by total intravenous anesthesia (TIVA) using a continuous infusion of propofol. However, a study showed that maintenance with propofol in septic female dogs resulted in higher hypotension compared to maintenance with isoflurane, indicating that it may not be the best modality for these patients.
Monitoring during and after the anesthetic procedure is very important, as sepsis has great potential to overload the cardiovascular system and decrease its ability to perfuse and oxygenate tissues. Therefore, it is crucial to monitor blood pressure, preferably invasively, as well as electrocardiographic tracing, capnography, and pulse oximetry.
Complications
Hypotension is the main complication observed in cases of pyometra, and that's why it's important to monitor blood pressure, preferably invasively if possible. To avoid hypotension, several maneuvers can be adopted. The first step is always to adjust the anesthetic rate (inhaled or intravenous) to the minimum necessary. If blood pressure is not normalized, the transanesthetic fluid therapy rate can be increased through fluid challenges or by raising the infusion rate. However, often there is a need for the use of vasoactive agents such as dopamine, ephedrine, or even norepinephrine to increase peripheral vascular resistance. The use of hypertonic solution is also applied in some cases.
So...
Pyometra is a complex and urgent situation, as it can pose significant risks to the lives of affected dogs. However, a well-executed pre-anesthetic approach, a properly planned anesthetic protocol, combined with careful and comprehensive monitoring, allow for anesthesia to be performed in these cases with greater safety.
Read also about:
- What are vasoactive substances and what are they used for?
- Acid-Base Balance #21
- Fluid Therapy - #22
Find out more:
Hesser A. Medical Management of Pyometra. WSAVA Congress, 2019.
Lima et al. Comparison of preoperative fluid therapy protocols associated with inhalational or total intravenous anesthesia for anesthetic procedures in dogs with sepsis. Braz J Vet Med, 44:e001222, 2022.
Mastrocinque S, Fantoni DTA. Comparison of preoperative tramadol and morphine for the control of early postoperative pain in canine ovariohysterectomy. Vet Anaesth Analg, 30:220-228,2003.
Nagashima et al. Microcirculation assessment of dexmedetomidine constant rate infusion during anesthesia of dogs with sepsis from pyometra: a randomized clinical study. Vet Anaesthe Analg. 49:536-545,2022.
Smith FO. Canine pyometra. Theriogenol, 66:610-61,2006.
Stone et al. Renal dysfunction in dogs with pyometra. JAVMA, 193:457-464,1988.
Suggestions? Thoughts? Comments? Share!






 Views Today : 95
Views Today : 95 Views Last 30 days : 4716
Views Last 30 days : 4716 Views This Year : 37333
Views This Year : 37333